Understanding cancer requires viewing it as a systemic disease, focusing not only on the malignant cells but also on the patient and the microenvironment in which the tumor develops.1
Primary and metastatic tumors are complex ecosystems composed of neoplastic cells, extracellular matrix, and “accessory” non-neoplastic cells, which include cells important for the tumor’s structure and infiltrating inflammatory immune cells. Thus, tumor development is fueled and shaped by the relationship between cancer cells and accessory cells, forming a highly specialized microenvironment characterized by chronic inflammation.2
Currently, it is known that when cancer arises in the body, it interacts with the immune system in such a way that:1
- Either the immune system is capable of controlling and destroying the cancer;
- Or the cancer stimulates the development of chronic inflammation and a microenvironment conducive to tumor growth, inhibiting its elimination by the immune system.
Immunosurveillance: Immune Response to Tumor Cells
The presence of inflammation in tissues can play a dual role. On one hand, activation of the immune system can eliminate tumor cells and prevent tumor development; on the other hand, the impact of inflammatory mediators can initiate and contribute to tumorigenesis.2
When antitumor mechanisms are effective, all known immune effectors (innate and adaptive) participate in the steps of tumor recognition and control. The sequence occurs as follows:1
- Natural killer (NK) cells detect the initial cancer cells through their antigens (specific proteins expressed by cancer cells).
- This leads to the destruction of some of these cells and the release of tumor antigens.
- Macrophages and dendritic cells process the fragments of the destroyed tumor cells.
- Upon activation, macrophages and dendritic cells begin to secrete pro-inflammatory cytokines and present tumor-derived molecules to T and B lymphocytes.
- The activation of T and B lymphocytes, in turn, induces these cells to produce more pro-inflammatory mediators.
- Activated B lymphocytes produce antibodies against tumor cells, while T lymphocytes recruit more T lymphocytes and secrete substances toxic to tumor cells.
- This response leads to the elimination of the remaining tumor cells and the generation of immunological memory to specific tumor components, preventing its recurrence.
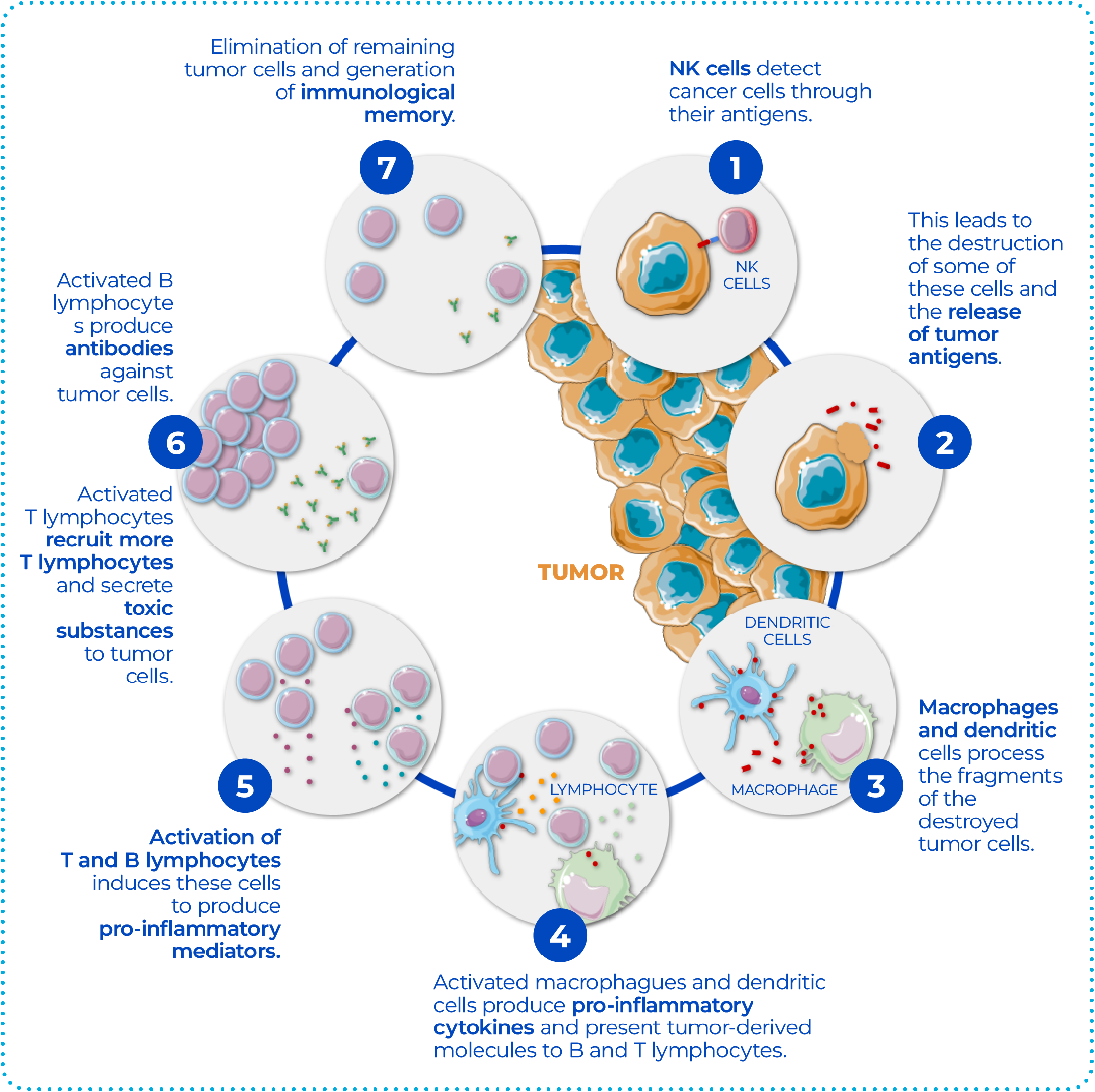
Figure 1. Sequence of steps involved in tumor recognition and control in antitumor immune mechanisms. NK: natural killer. (Adapted from Finn OJ. Ann Oncol. 2012;23 Suppl 8:viii6-9.1)
Through the process of immunosurveillance, the immune system can identify and eliminate tumor cells. That is, a highly immunogenic cancer (which expresses specific tumor antigens) in a highly immunocompetent person will result in appropriate stimulation of the innate immune system, with the production of highly immunostimulatory cytokines, inflammation, activation of a large number of T and B cells, leading to the immediate elimination of any emerging tumor.1
However, in cases where the immune system is not able to completely eliminate the cancer, a state of equilibrium develops in which the tumor does not progress or metastasize. This is a period during which its slow growth is accompanied by repeated activation of the immune system, leading to the elimination of some cancer cells, followed by other cycles of tumor growth and partial destruction.1
Eventually, if the immune response fails to completely eliminate the tumor, natural selection occurs for cancer cells that can resist, evade, or suppress the immune response, leading to tumor escape and its progressive growth. These cancer cells adopt various mechanisms that lead to peripheral immune tolerance, where the immune system no longer recognizes them as foreign elements to the body. Additionally, they recruit immunosuppressive cells that inhibit other tumoricidal cells, further suppressing the innate anticancer immune response.1,2
Based on this knowledge, immunotherapy was developed, aiming to modulate immunity in the tumor microenvironment to alter the immune response that is favorable to tumor promotion, making it favorable to tumor rejection, thereby providing cancer control.¹

Tumor Escape
According to MeSH, one of the main health descriptor databases maintained by the National Institutes of Health (NIH) in the United States, “Tumor Escape” can be defined as:3
“The ability of tumors to evade destruction by the IMMUNE SYSTEM.”
To avoid their elimination by the immune system, tumors develop immune escape mechanisms involving (Figure 2):4
- Loss of antigenicity.
- Loss of immunogenicity, with the gain of additional immunosuppressive properties.
- Creation of an immunosuppressive microenvironment with the recruitment of an immune response (with immunosuppressive leukocytes) that suppresses antitumor immunity.
Thus, the emergence of cancer appears to be related to an immune system that actively selects tumor clones that are poorly antigenic, poorly immunogenic, and/or establishes a microenvironment that suppresses productive antitumor immunity.4
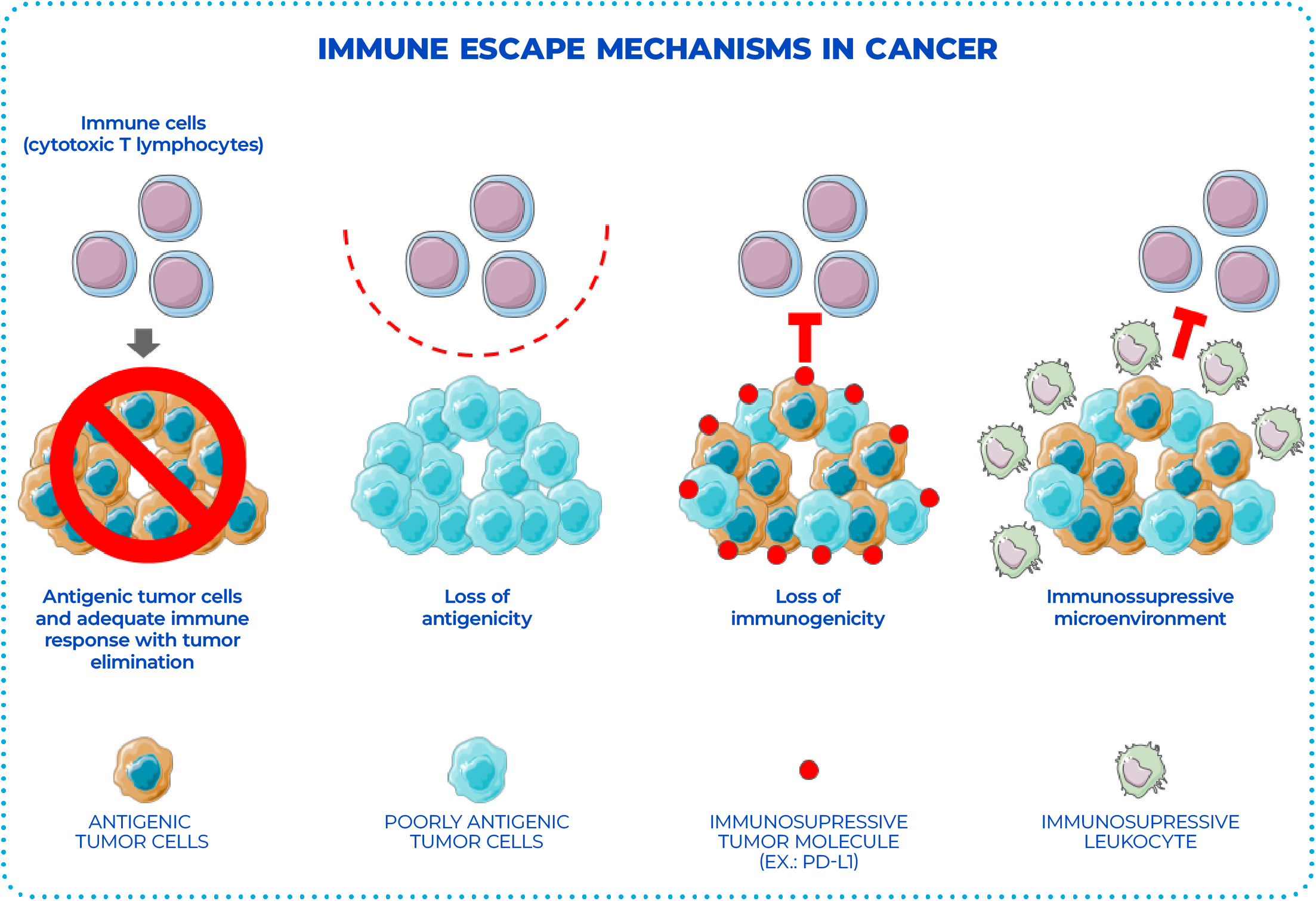
Figure 2. Immune escape mechanisms in cancer. (Adapted from Beatty GL et al. Clin Cancer Res. 2015; 21(4):687-92.4)
Loss of Antigenicity
Cancers can express a variety of non-mutated and mutated antigens that have the potential to induce specific immune responses against the tumor. However, to avoid immune-mediated elimination, cancer cells can lose their antigenicity through:4
- Selection of cancer cell clones that lack or have mutated immunogenic tumor antigens; or
- Acquisition of deficiencies in antigen presentation (e.g., loss of major histocompatibility complex expression, MHC, or deregulation of the antigen processing machinery).
As a result, immunogenic peptides are no longer presented, and there is no formation of the peptide-MHC complex responsible for the recognition of cellular antigens.4
Thus, the ability of the immune system to distinguish between normal and malignant cells is fundamental for cancer immunotherapy and depends, in part, on malignant cells retaining sufficient antigenicity. As a result, knowledge of the antigenicity of malignant cells can inform the potential susceptibility of a cancer to immune elimination by endogenous T cells. However, since malignant cells among patients and even within the same patient can be quite different, it is still unclear how to effectively quantify the antigenicity of a cancer.4
Loss of Immunogenicity or Development of Immune Tolerance
Tumors that retain sufficient antigenicity for immune recognition may escape elimination by decreasing their immunogenicity. In this way, immune tolerance is an important mechanism involved in the inhibition of the immune response, which can be triggered through immune checkpoints.2,4
The two best-described checkpoint molecules, CTLA-4 and PD-1, act as negative regulators of T-cell function and are associated with immune evasion of cancer. For example, the stimulation of the immunoinhibitory molecule PD-L1 on the membrane of cancer cells and its interaction with PD-1 (expressed by cytotoxic lymphocytes) results in the suppression of T-cell activity and inhibition of their antitumor activities (such as T-cell migration and proliferation, secretion of cytotoxic mediators, and cell death) (Figure 3A).2
Tumor Microenvironment
Although the immune response may initially act to inhibit tumor development, increasing evidence suggests that, in some tumors, tumor-infiltrating leukocytes can coordinate an “immune-privileged” microenvironment that impairs the productivity of antitumor immunity. That is, some tumors can maintain sufficient antigenicity and immunogenicity but avoid immune elimination by orchestrating a suppressive microenvironment. Supporting this hypothesis, strategies that eliminate populations of immunosuppressive cells and reverse immunosuppression have been found capable of restoring the ability of T cells to mediate antitumor activity.4
Immunotherapy
The increased understanding of the multiple immunological mechanisms for tumor elimination has made it clear that different immunotherapies depend on the patient’s immune system for long-term control or complete elimination of the tumor.1
Therefore, for tumors that retain sufficient antigenicity and immunogenicity, immunotherapy will need to focus on strategies that enhance:4
- Tumor-specific immunity (e.g., vaccines and/or adoptive therapy with tumor-infiltrating lymphocytes); and
- The killing of tumor cells by T lymphocytes (e.g., immune checkpoint blockade).
Over the past few years, the use of immune checkpoint inhibitors, such as anti-PD-1, anti-PD-L1, and anti-CTLA-4 (Figure 3B), has achieved remarkable success, increasing the antitumor response observed clinically, especially in melanoma and lung cancer, but also in other types of cancer.2

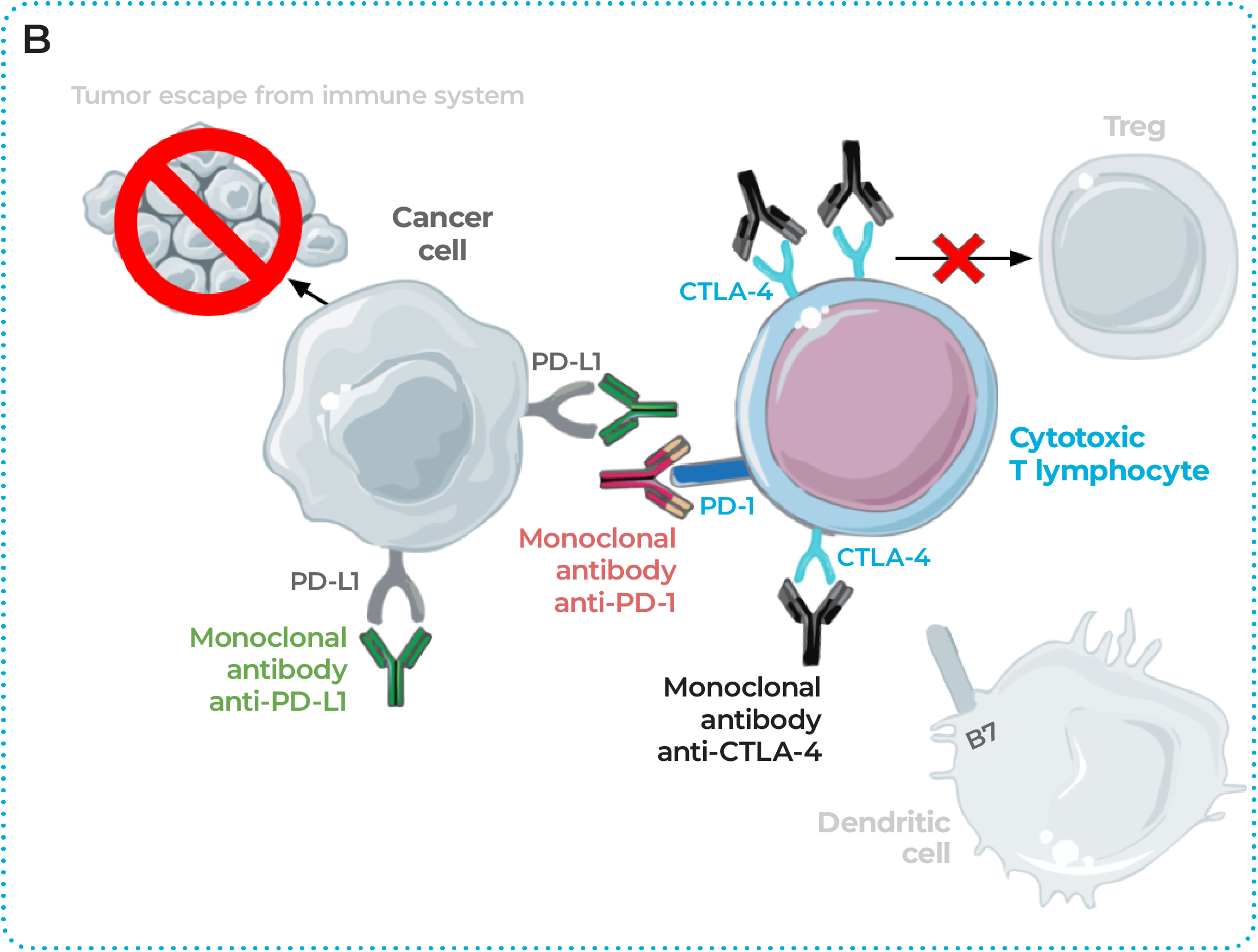
Figure 3. Mechanisms of tumor escape and the use of immune checkpoint inhibitors in cancer treatment. (A) The activation of cytotoxic T lymphocytes in the tumor microenvironment is important for the elimination of cancer cells. However, this mechanism can be inhibited through (1) immune checkpoints or (2) the suppressive effect of regulatory T cells (called Tregs). These checkpoints are formed by molecules that bind to receptors on the cells, and when this binding occurs, it’s as if the defense cell receives a message to deactivate its action. In cancer, the activation of immune checkpoints allows cancer cells to escape immune attack, survive, and grow. When PD-1, a protein expressed on T lymphocytes, binds to its ligand PD-L1, expressed by cancer cells of different tumors, it sends a message to T lymphocytes to stop their cytotoxic action against tumor cells. Tregs have their activity increased by another protein found on T lymphocytes, CTLA-4, leading to suppression of immune activity. Furthermore, when CTLA-4 is bound to a protein called B7, inhibition of the T cell itself occurs, preventing it from killing cancer cells. In other words, the activation of CTLA-4 causes T lymphocytes to stop fighting the tumor. (B) In turn, pharmacological inhibition of these immune checkpoints with monoclonal antibodies restores the antitumor activity of cytotoxic T lymphocytes and interrupts immunosuppression. Abbreviations: CTLA-4: cytotoxic T-lymphocyte antigen 4; PD-1: programmed cell death protein 1; PD-L1: programmed death-ligand 1; Tregs: regulatory T cells. (Adapted from Ayoub et al. Breast Cancer 2019;11:53–69 5)
However, it is likely that these approaches have limited efficacy for tumors that contain defects in antigen processing and presentation and, therefore, cannot be recognized by T cells. For these tumors, strategies that may be more effective are those that redirect innate immunity with antitumor properties (e.g., natural killer cells and macrophages) or, alternatively, cellular therapy using T cells engineered to express chimeric antigen receptors (CAR). In this type of treatment, a patient’s T lymphocytes are modified in the laboratory to recognize specific tumor proteins, a method that may be more effective because it does not depend on antigen presentation restricted to MHC.4
Conclusions
Cancer is a complex disease that is established through various mechanisms, with a special relationship with the immune system, which initially has the ability to combat neoplasms. However, some tumors exhibit mechanisms to escape the immune system, enabling the development, progression, and metastasis of cancer. Based on this knowledge, various immunotherapies have been developed and are being used, and today, oncoimmunology is a a rapidly evolving field, with substantial advancements already reflected in clinical outcomes and patient survival rates.1,2,6
Bibliographic references
- Finn OJ. Immuno-oncology: understanding the function and dysfunction of the immune system in cancer. Ann Oncol 2012;23 Suppl 8:viii6–9.
- Gonzalez H, Hagerling C, Werb Z. Roles of the immune system in cancer: from tumor initiation to metastatic progression. Genes Dev 2018;32(19-20):1267.
- Tumor Escape – MeSH – NCBI [Internet]. [cited 2022 May 16];Available from: https://www.ncbi.nlm.nih.gov/mesh/?term=tumor+escape
- Beatty GL, Gladney WL. Immune escape mechanisms as a guide for cancer immunotherapy. Clin Cancer Res 2015;21(4):687–92.
- Ayoub NM, Al-Shami KM, Yaghan RJ. Immunotherapy for HER2-positive breast cancer: recent advances and combination therapeutic approaches. Breast Cancer 2019;11:53–69.
- Loose D, Van de Wiele C. The immune system and cancer. Cancer Biother Radiopharm 2009;24(3):369–76.